Connecting Science & Health
WE live in a time of great knowledge and of great change.
With our current understanding of the environmental and socioeconomic challenges we will face in the coming decades, we need to do better and work harder to create equitable societies, around the world.
Graduate level education in Science trains us to be both visionaries and skeptics.
Science, i.e., the scientific process, is a socialist process also. We share our knowledge with colleagues and hope that their assessments lead to concordance, with regard to primary findings.
As more and more people agree with the claim, the field of study moves from the domain of hypotheses (speculations) to the realm of theories. Theories represent the primitive (fundamental) structure of Reality, the reality we share. They give rise to Technology.
Every claim that is published in a peer reviewed journal, and especially significant findings that reach the level of an established Theory, will be challenged.
Notable examples are Einstein’s General Theory of Relativity and the Quantum Mechanical (QED) model of the atom developed by Neils Bohr and fellow physicists. These are well established foundations of modern physical science that are about a century old.
Verifications, i.e., checks of concordance between experiment and theory (model), extend beyond the ninth decimal place. These processes mature the field and move it from producing heat to one producing light.
Though challenges continue, these models have not failed. They operate above the Six Sigma manufacturing quality guideline required to sustainably produce the high tech wonders from our electronics and telecom sectors.
By contrast, conventional medicine practices operate at the 1-2 sigma level, i.e., opinions. Looking for a cure is often a hit or miss process, with ~50-70% chances for a complete cure, often following serial and unsuccessful pharmacotherapies which may last years or decades.
Lots of room for improvement, if we really want to invest in The People, and advance the scientific basis for modern healthcare.
I started formal studies in health and medicine following a long career in physical and analytical chemistry. As such, I think most drugs that survive rigorous clinical evaluations and are released for general use can be helpful, if used properly. If they are used properly.
Research has identified multiple adverse drug-drug interactions via our endogenous drug detox processes, e.g., through CYP450 induction or inhibition, as a significant cause of morbidity in conventional care, potentially leading to increased mortality. A weakly funded Drug Induced Liver Injury Network (DILIN) desperately seeks more input from clinicians.
The scope of scientific contributions that can improve human health is vast. However, its primary toolkit has been neglected in the American healthcare system. More specifically, an inexplicable and persistent inability to use the scientific method to distinguish effective from ineffective clinical practices. It appears to be a fundamental gap in clinician training, both during graduate school and subsequent clinical/professional practices.
This lapse can be easily corrected by requiring post graduate continuing education credits, where practicing clinicians learn to
1) formulate a hypothesis, e.g., supporting long term opioid use, without data, is a classic 21st century example of microcephalic doctoring
2) design/develop the analytic techniques that will be used to collect relevant patient data
3) carry out evaluations & statistical analyses needed, and
4) declare/demonstrate the outcome of their investigation.
If this undergraduate level training had been required for medical doctors currently in practice, we could have avoided the carnage…, the ongoing economic and health disasters associated with the opioid epidemic that continue to this day.
Licentious and scientifically indefensible prescribing practices still flourish today, promoted by some legislators in the name of taxpayer support for the Pharma sector, an integral component of the Medical Industrial Complex.
Current published analyses show that the U.S. Pharma sector has been generating twice the profit of other manufacturing operations over the last decade, without taxpayer subsidies.
The People pay trillions of dollars every year for these agency level lapses to ensure quality.
The United States Health & Human Services’s (HHS) inability to think clearly, i.e., selecting long term outcomes favoring the taxpayer, is responsible for an overpriced healthcare system that wastes 30-40% of their budget every year by paying for clinical services that do not benefit the patient. In 2024, that is ~ $1.5 trillion.
Could America use $1.5T annualy for societal uplift programs?
Our bloated and inefficient care system looks incompetent, by widely accepted measures of clinical performance with regard to public health, relative to other industrialized nations, e.g., EU.
How doctors buy their way out of trouble
Medical doctors are famous for claiming that only they know what is best for patients, on account of a “special” awareness which cannot be documented scientifically or otherwise discussed.
The continuous whining I hear about current documentation requirements, i.e., electronic health records(EHR), suggests that recognizing the importance of appropriate documentation of complex (expensive) interventions is not a strength in the medical doctor community.
Multiple news paper articles have showcased how colleagues(MD) often close ranks to support indefensible and unsustainable practices, as noted recently with regard to allegations of CMS fraud involving unnecessary procedures. Medical doctors apparently cannot be held to any professional standards for the services they provide.
One settlement agreement (see link) included a signed acknowledgement that one of the medical doctors had performed and billed for surgical procedures based on symptoms that were “insufficient to justify these treatments.” However, they could not be indicted, a reflection of the dictatorial tendencies we see in medical doctors.
Medical doctors are the “entitled” in CMS programs, not the poor and indigent people whose need for healthcare border on crises, while struggling (working) with multiple jobs to take care of themselves and their families.
We must acknowledge that medical doctors are too well paid (~$500K/yr) to rock the boat of revenues generated by regularly writing lifetime prescriptions (No Cures Here) and then recommending expensive corrective procedures when the drugs fail to cure or prevent disease.
Current escalatory prescribing practices include a rising tide of medications, affecting both Body and Mind via metabolic and psychotropic actions, because one drug is often not enough. Rather than acknowledging diagnostic errors, the initial ‘honeymoon’ phase of the therapeutic alliance involving serial drug therapies is often followed by abrupt discontinuations of opioid and narcotic drugs, following anticipated threats of regulatory (PDMP) review. Following multiple failed pharmacotherapies, patients may be advised that aggressive or surgical (expensive) interventions will now be needed.
There is more money for a clinic/hospital in performing a single surgical intervention for pain management than 100 sessions of acupuncture. For this reason, they collect minimal data on the comparative efficacy of nonpharmacological vs surgical interventions.
Based on our entrenched sociocultural perspectives favoring drugs over nondrug therapies, medical doctors can do no wrong. For example, there are no International Classification of Diseases (ICD-10) codes for Deaths due to Medical Errors. Recently (2017), medical errors in the United States were recognized by researchers as the third largest cause of patient deaths, at ~500K deaths/year.
As lawyers will tell you, if you didn’t collect the data, medical errors don’t exist. No statement or dissent from HHS followed the release of the 2017 article, suggesting that the estimates were accurate, or even an undercount, as some analysts suggest.
Can you imagine what would happen if our police killed 500 000 people every year and had nothing to say for themselves?
A glaring example of incompetence
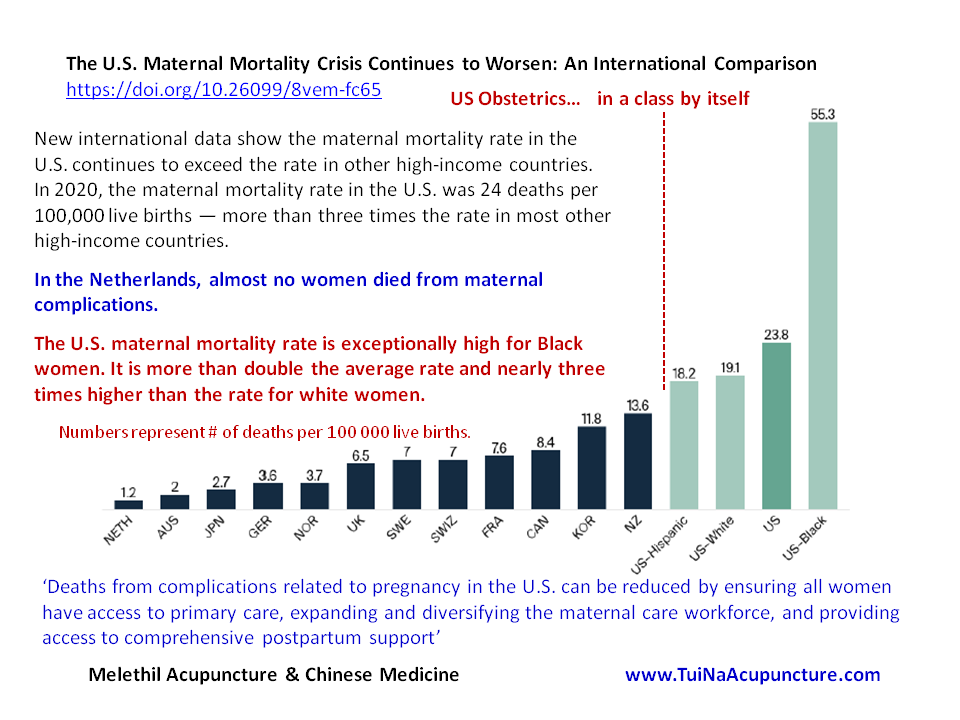
No US obstetricians, or HHS agency staff, are willing to go public and explain why so many American mothers die or have other adverse outcomes during childbirth. Much more so for African Americans. How come every other nation (slide) does better? Absolutely shameful.
Investigations by overseas research groups suggest that a proximate cause for these tragedies lies rooted in current hospital (clinic) delivery practices. More specifically, they treat the prospective mother as a widget to be “processed” most efficiently, with a manufacturing mindset.
Clinics and hospitals that depend on Public Care programs (CMS funded) operate freely with frequent disclosures of reductions in frontline care staff. Minimization of effort and the maximization of revenues for their birthing and post natal services, provided for both mother and child. Outcomes?
The People have to wake up and take charge of their health goals and objectives, i.e., increase Health Literacy. There is a storm brewing.
The primary areas that need attention in industrialized nations are lifestyle choices and practices, involving proper nutrition and age- & health- appropriate physical and social activities. In less developed nations in Africa and Asia, the long term unmet needs for food and shelter, are leading many people to experience widespread starvation and other serious health risks, e.g., infectious diseases.
Global warming, aka Climate Change, is not expected to improve our circumstances.
WE can change our health outcomes, if we want to. There are many community resources that can help.
Alternative Perspectives
For thousands of years, Asian traditions of health pointed out the importance of patient engagement in directing their own healing. We are talking about culturally aware integrative health (IH) practices that are built on healthy lifestyles, practices tested and defined over millennia. More specifically, in Ayurveda, we have Yoga, and in TCM we have chi kung or internal bioenergy (electricity) practices, known as Neidan / Internal Elixir techniques.
These practices have 2000+ years of evidence to support their self directed use for long term health, without fostering drug dependencies. However, a pattern of monolithic ethnocentrism, i.e., the cultural impoverishment, demonstrated by arrogant and ignorant medical doctors, prevents their formal inclusion as important aspects of health related services Western societies.
WE continue to pay a heavy price, in blood and treasure, for the centuries long ill advised government policies that neglected the relevance of multicultural diversity in creating stable societies for the long term, i.e., more than 200-300 years.
Well past the middle of the 20th century, the United States envisioned itself to be a nation reserved primarily for the descendants of the North European cohorts that plundered the Americas, starting five centuries ago.
There are no terminal degrees in Asian Internal Elixir (Neidan) disciplines and the practices extend along one’s life trajectory, offering age appropriate workarounds for failing bodies.
Learn to control time (personal), rediscover the beauty of the gifts from the natural world every day. Celebrate Life, as the visionary poet William Blake noted so long ago (Auguries of Innocence).
In internal awareness practices, we ‘shrink; our Mind to gain access to communications between our Body & Spirit (Society, for those existing primarily on the material plane), and our attention is drawn inward, through a perceptual doorway known to yogins as “Starving of the Senses”. Many are blocked in accessing this internal power, because of unresolved internal disharmony.
Shamanic practices apparently recognize these transitions as an important aspect of self development and gaining (in)Sight.
My research on mood disorders suggests that many who suffer are Seekers on a path of self discovery who are unable to transit through this “inner gate” to realize the outcomes of focused attention, i.e., Self Realization.
One well known goal of Inner Energy cultivation practices, around the world, is to abolish the dichotomous thinking that frames human identity. This goal is known by various names– as moksha, nirvana, satori, and also as finding Beloved, in the mystical traditions of the world.
These journeys may be facilitated using a teacher-disciple relationship, the guru-shishya paramparya in the Vedic traditions, built on shared values that lead to a lifelong connection. As the connection grows stronger, there is less need to talk.
With dedicated and consistent practice, as our self awareness and confidence (swashakti) grow, we begin to see ourselves more clearly, how our thoughts and actions have led us to where we are today, and to where we are going. We understand how to change, when needed, under our own direction. This is Resilience.
Many forms of talk therapy, including prayer, have also been used to support these transitions. All of them recognize that personal effort (practice) is the primary determinant of success, Change.
ParaphrasIng from the Daoist traditions, … when the Great Work is done, The People shall say we did it all by ourselves.
Borrowing from the Yoga (Vedic) traditions, Realize the Healer Within.